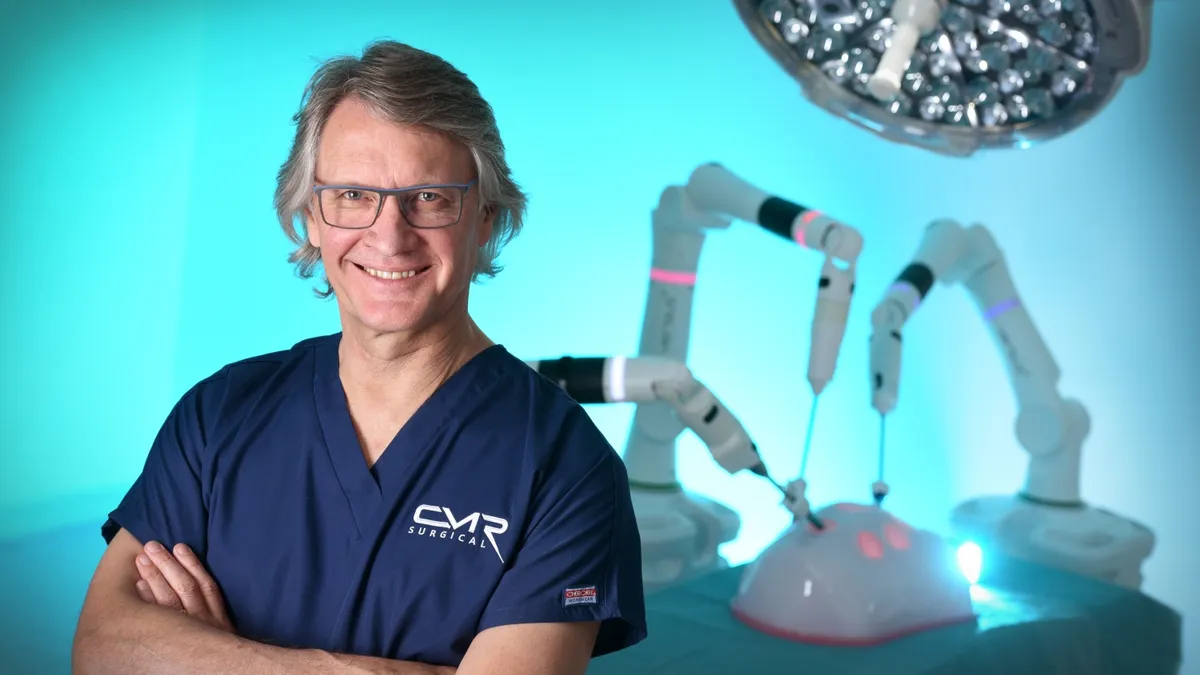
CMR Surgical is taking on Intuitive Surgical in the U.S. after gaining a de novo authorization in October for its Versius robot, challenging the market leader’s 20-year dominance in soft tissue robotic surgery.
In competing with Intuitive on its home turf, UK-based CMR has pulled ahead of Medtronic and Johnson & Johnson, whose soft tissue surgical robots are not U.S.-approved. Versius’ first indication is in gallbladder removal surgery, with more procedures expected to follow.
“This competition, it’s good for health. I don’t think a monopoly market is healthy,” said Mark Slack, CMR co-founder and chief medical officer. “There will be 3-4-5-6-7 providers in due course.”
Slack said users are attracted to the Versius robot’s flexible design and smaller-sized instruments. He is not fully sold on force feedback sensing as a robot advantage and would like to see more data in general on how well surgical robots are performing. CMR’s robot will also compete on price, Slack said.
Slack discussed the Versius system’s attributes and the advantages and challenges of robotic-assisted surgery in a conversation with MedTech Dive.
This interview has been edited for length and clarity.
MEDTECH DIVE: Why did you choose to introduce Versius in multiple global markets before focusing on the U.S.?
MARK SLACK: Largely picking a fight we could win. There's an 800-pound gorilla in the room called Intuitive. It is uniquely successful. Not ever in medtech has there been a single company that’s had such a monopoly on any subject.
They brought the robot out in [2000], and the first robot to compete with them, the first competitor, was us in 2019. So they're 20 years just running. To go head-to-head with them in their own backyard is pretty damn dangerous. And so, we wanted to get established. We wanted to do more clinical development.
I also have a great belief that if you are going to be successful with medical technology, it's got to be not just for the high-income countries. If we’re saying that's the best standard of care, then that should be hopefully translated to all other communities around the world. That's where I started. But you can't stay out of America with health. So yeah, time to join in.
I don't think Intuitive will be particularly delighted with us coming.
How will Versius compete against Intuitive’s da Vinci?
It's a smaller robot, it's modular, it's more transportable. It can be packed out of the way when not using it. The modularity and affordability are really important.
When you have six, seven or eight robots in a hospital, which is the way it's going, where do you put them, if they're very big, when you're not using them? You actually close theirs down when you're not using them, whereas ours can be put against the wall, in a cupboard, etc. It's easier to store and therefore doesn't occupy large amounts of space in a hospital or shut down your theaters.
From the point of view of staff being open, being able to talk and communicate, the modularity is hugely important. The nurses 100% want to be in interaction with the surgeon, and the anesthetists want their open console.
And then finally, we have smaller instruments than the other robots, and that means that we perform pretty well in small spaces.
Ultimately we will compete in all operations, but there will be areas where we really do shine, like the chest, or in children, where the anatomical spaces are smaller, which actually favors the smaller robot.
Do you expect some hospitals to add a Versius robot while also continuing to use da Vinci?
We see it already. We have a number of hospitals in the UK that have both, and some surgeons like the one and others like the other one. That still is a war that needs to be played out.
It's unlikely that you'll ever get an instrument that everybody thinks is the best, and there will be strengths and weaknesses. Over time, as we play it out, and as we do more research and we get the data, we'll see where we absolutely shine, and we'll see areas where we are equivalent, and then possibly areas where it might be superior.
You notice I said might.
We have some centers where people have done 1,500-2,000 cases on our robot and really gained extensive experience. We have some users in the U.S. who are genuinely waiting for us because they feel we are the right size. They are very keen that that might be a better way of doing robotic surgery.
One talked-about feature of Intuitive’s new robot, da Vinci 5, is force feedback that lets surgeons sense pressure on tissue at the tip of an instrument. Is that something you will offer?
We've got to be sure of what's real in terms of advantages and what's not. We actually have force feedback on our robot, and we choose not to activate it at the moment. I'm partly the reason for that. I'm not 100% convinced that it does improve things.
I think force feedback has a way to go to be really useful. And you know how many hundreds of thousands of cases have been done robotically with outcomes better than laparoscopic surgery with no force feedback, and that's the da Vinci figures.
And then all the other features, it's how much of it is marketing and how much is real? And that's what I would like to see more in robotics: less hype and more fact. What is the satisfaction rate? What is the success rate? What are the false negatives and the false positives and so on. Those are all really, really important things that we need to be a little bit more medical about as we go forward. Otherwise, the whole health system just becomes more and more expensive and not necessarily better.
Is robotic-assisted surgery better than laparoscopy?
That's a very important point to decide. If you asked me, at the moment, to debate that robotics is better than laparoscopy, I would be pretty cautious. If you take a really skilled laparoscopic surgeon, the chance that the robot will necessarily do it better than them is quite slight, because they are fast, they are able, and they are very good at it.
However, we are now starting to see data from areas where the robots are performing better than laparoscopic [surgery]. Watch the space. I think you may well find superiority in robotics over laparoscopy.
I believe I can train a person on robotic surgery far quicker than I can train a person for laparoscopy, and better. We’ve got data to support that. If I was going to teach you — you may be a very skilled laparoscopic surgeon — to tie a knot laparoscopically, that's about 50 or 60 hours worth of training. I reckon on a robot I could teach you in about an hour.
If I had a crystal ball, in 10 years time, I think we will be showing the advantages of robotics over laparoscopy.
What other indications are you pursuing, and how is that process going?
We chose to go in the most efficient route possible, both financially and time-wise, which is to do a de novo and therefore only chose limited clinical indications. The idea being, once we get that, we'll then [submit 510(k) applications] on multiple other clinical scenarios. We'll start by upgrading the system, and then we'll do colorectal, thoracic and all the other specialties, one after the other.
The real achievement was getting the system past a full FDA approval for the system and for all our instruments, because then doing the 510(k) is altogether much easier. So we do small, limited clinical trials and expand it across to the other specialties here.