New medical devices are reshaping the medtech industry
Boston Scientific's Farapulse pulsed field ablation system is one new product that is changing how physicians treat atrial fibrillation.
Permission granted by Boston Scientific
Note from the editor
New technologies fuel the medical device industry. Whether they’re cardiac devices or wearable diabetes technology, products can shift markets or create new ones that boost companies’ businesses.
Over the past several years, multiple new products have reshaped the medtech industry. For example, pulsed field ablation devices from companies like Boston Scientific and Medtronic have changed how physicians treat atrial fibrillation, and provided strong sales that have grown both companies’ electrophysiology portfolios. The excitement about PFA has drawn other top medtech companies to compete for market share, including Johnson & Johnson and Abbott.
Renal denervation is another topic getting a lot of attention. The hypertension treatment has a potentially huge addressable market, and cardiologists have advocated for broader coverage of the treatment.
Other areas where new products can disrupt established markets include surgical robotics, where smaller firms are racing to launch their soft tissue robots to compete with longtime leader Intuitive Surgical. However, Intuitive’s da Vinci 5 robot may be enough to hold them back.
Meanwhile, Dexcom and Abbott have developed over-the-counter glucose sensors — a first in the space — that are attracting users who do not have diabetes and are using the sensors as wellness devices.
There are a lot of exciting new technologies in the medical device industry, and likely more to come in the next several years. Read more to see which ones could shake up the current landscape.
The Food and Drug Administration has authorized more medical devices that incorporate artificial intelligence. Keep track of the latest developments in this database.
By: Elise Reuter and Jasmine Ye Han• Published May 20, 2025
Artificial intelligence has become a buzzword in the medtech industry as more medical devices incorporate the technology. Device companies are using AI to speed up imaging, triage CT scans for serious conditions and identify potential heart arrhythmias.
The Food and Drug Administration is also fielding more submissions in recent years, with the 235 AI devices authorized in 2024 being the most in the agency’s history. As of the FDA’s latest data update in July 2025, the device center had authorized more than 1,200 AI devices since 1995.
The majority of AI devices are in radiology, but the technology is becoming more prevalent in other specialties, such as cardiology and neurology.
Regulators face a challenge as generative AI, which can create text and images, and foundation models, large-scale models that can be used for numerous purposes, gain traction among developers.
MedTech Dive is tracking the FDA’s list of authorized AI technologies to understand which companies are developing the most AI devices and how those products are used.
Devices authorized by the FDA from 1995 to July 10, 2025, which include hardware or software features.
Methodology:
MedTech Dive downloaded the FDA’s list of AI/ML-enabled medical devices on July 31, 2025. The FDA last updated the database on July 10, 2025. The FDA compiled the list using product codes and device summaries. The list is not exhaustive, but it is intended to represent devices that incorporate AI/ML across medical disciplines, the agency said. The definition of a device includes hardware and software features. The FDA sometimes adds older devices to the list.
MedTech Dive collected information on each applicant and whether a company was acquired for its analysis. In cases where a company was acquired multiple times, the most recent parent company or majority owner was listed. One exception is Siemens Healthineers, which is majority-owned by Siemens. Parent companies were defined as firms that make a product, and private equity and investment firms were not listed.
MedTech Dive also collected classification information from each filing to provide a description of each device. In a few instances, the classification field is empty because the filing didn’t contain that information.
We made edits to reflect MedTech Dive’s editorial style.
Article top image credit: Courtesy of GE Healthcare
Renal denervation gets strong backing from cardiologists ahead of Medicare coverage decision
Doctors told the Centers for Medicare and Medicaid Services that more patients need access to the procedure, with one calling it the start of a new era in hypertension management.
By: Susan Kelly• Published Sept. 4, 2025
Cardiologists are welcoming the arrival of a new device-based hypertension treatment called renal denervation and asking Medicare to cover the procedure for a large patient population.
Doctors, medical groups and others have endorsed national reimbursement for renal denervation in dozens of public comments submitted to the Centers for Medicare and Medicaid Services ahead of a final Medicare coverage decision expected by early October 2025. Many cite concern about the high numbers of patients whose blood pressure remains poorly controlled despite the availability of multiple drug treatments.
Roughly three-quarters of U.S. adults with hypertension do not have it under control. Writing in favor of the national coverage determination, or NCD, physicians recounted seeing first-hand the consequences of uncontrolled blood pressure in patients who suffered stroke, heart attack, heart failure and kidney disease. The doctors view renal denervation as a much-needed option to stop the progression.
“Renal denervation (RDN) represents a significant breakthrough, providing a novel tool to lower blood pressure and reshape long-term outcomes in ways that once seemed out of reach,” Oluwaseun Akinseye, an interventional cardiologist at Methodist Le Bonheur Healthcare in Memphis, Tennessee, said in comments to the CMS.
In late 2023, the Food and Drug Administration approved two renal denervation devices: Medtronic’s radiofrequency-based Symplicity Spyral and Recor Medical's ultrasound-based Paradise system. Limited insurance reimbursement, however, has slowed clinical adoption.
The CMS NCD is expected to accelerate use of the minimally invasive procedure for patients whose blood pressure hasn’t improved despite lifestyle changes and medications.
In their comments to the CMS, numerous cardiologists described positive early experiences with the procedure.
Eric Secemsky, of Beth Israel Deaconess Medical Center and Harvard Medical School, said all of the more than 30 patients treated with renal denervation in his multidisciplinary hypertension program were discharged the same day without procedural complications and had sustained blood pressure improvement.
“Our only significant barrier to date has been the lack of reimbursement,” Secemsky told the CMS.
Omar Hyder, from the Brown University Health Cardiovascular Institute, described the treatment as safe, straightforward and extremely effective, after performing just over 20 procedures. “In a subset of patients,” he noted, “we have seen even more drastic reductions in blood pressure requiring the weaning of medications.”
The long road to approval
During a renal denervation procedure, energy doses are sent to ablate overactive nerves near the kidneys that contribute to high blood pressure. The reduced nerve activity causes a drop in blood pressure.
While physician interest in the technology is growing, its potential for success was not always clear.
Medtronic’s work on renal denervation picked up steam with the 2011 purchase of Ardian, developer of the Symplicity catheter. Along the path to FDA approval, the treatment faced research setbacks that triggered considerable debate about its effectiveness.
The proposed NCD, along with new hypertension treatment guidelines from the American College of Cardiology and American Heart Association, validates renal denervation as an additional option for managing hypertension in patients who do not sufficiently respond to lifestyle modifications and pharmaceutical treatments, a Medtronic spokesperson said in an email.
“The proposed NCD represents a novel, meaningful market for Medtronic,” the spokesperson said. "To date, we are seeing great interest from healthcare systems across the United States that are looking to offer the Symplicity blood pressure procedure."
Both ablation methods — ultrasound and radiofrequency — won FDA authorization despite demonstrating only modest reductions in absolute blood pressure values in their phase 3 clinical trials, said Stanford University School of Medicine’s Vivek Bhalla. But the data are noteworthy, he wrote, because “even a modest reduction has a substantial effect on lowering cardiovascular risk.”
Furthermore, subsequent registry data point to a sustained drop in blood pressure over time, wrote Bhalla and other doctors.
“Reimbursement for these procedures is a necessary step to translate these research studies to the broader public to improve the woefully poor rates of blood pressure control in the United States,” Bhalla told the CMS.
Real-world care
Michael Rosenberg, who has performed about 30 renal denervation cases over the past year using Recor’s device, said the research to date has not told the whole story.
“Results have been better than the literature has suggested and patient satisfaction has been very high. I would say it has been a resounding success from the standpoint of patient welfare, outcome, and safety,” said Rosenberg, an interventional cardiologist at Froedtert South Medical Center in Kenosha, Wisconsin.
A recurring theme from supporters of the procedure centered on how high blood pressure should be defined, with many arguing the CMS’ proposed threshold of 140/90 mm Hg is too restrictive.
In comments to the CMS on the NCD, the ACC, Society of Cardiovascular Angiography & Interventions, and Society for Vascular Medicine jointly recommended the agency adopt a definition based on systolic blood pressure greater than 140 mm Hg, without a diastolic requirement, to avoid excluding patients with isolated systolic hypertension, which is common in older adults.
The groups, along with many doctors, also urged greater flexibility in requirements for medication timelines, doctor visits, and multidisciplinary hypertension screening and treatment programs.
Araya Negash, an interventional cardiologist at Corewell Health in Grand Rapids, Michigan, cautioned against adopting policies that could inadvertently limit treatment only to those with the means to seek out specialized services.
“As we enter a new era” in hypertension management, wrote Negash, “it is essential that we balance innovation with equitable access to ensure that all patients who could benefit from this therapy are able to receive it.”
Article top image credit: Courtesy of Medtronic
Abbott and Dexcom are launching the first over-the-counter CGMs. Here are 7 questions on the new tech.
Experts expect the release of new over-the-counter glucose monitors in the U.S. to fuel more widespread use of the devices.
By: Elise Reuter• Published June 26, 2024
The first over-the-counter glucose sensors will launch in the U.S. in summer 2024. Dexcom and Abbott received Food and Drug Administration clearance for OTC continuous glucose monitors in March 2024 and June 2024, respectively. Although the devices use the same hardware as past CGMs, they’re intended for a different group of users — people who do not take insulin.
Dexcom is targeting people with Type 2 diabetes who don’t take insulin with its new Stelo device, although Stelo can also be used by people who don’t have diabetes, thanks to a broad label from the FDA. Abbott, meanwhile, will split its over-the-counter products into two sensors: Lingo, which is intended for people who don’t have diabetes, and Libre Rio, which will compete more directly with Dexcom for Type 2, non-insulin users.
The new devices could allow the companies to reach about 25 million people in the U.S. with Type 2 diabetes who don’t take insulin, 15 million people who have been diagnosed with pre-diabetes and an estimated 85 million people who have undiagnosed pre-diabetes, William Blair analyst Margaret Kaczor Andrew said in an interview.
MedTech Dive spoke to experts about what to expect from the three product launches.
When will the devices be available and how much will they cost?
Dexcom is planning a late August 2024 launch of its Stelo sensor, Chief Operating Officer Jake Leach said in an interview. Dexcom will first sell the devices online, which Leach said will help the company learn more about users and their buying patterns, although he sees “great opportunity in other methods of distribution.”
Abbott also plans to sell its wellness-oriented Lingo device in summer 2024 through an e-commerce website. It has not yet disclosed timing for Rio.
Neither Abbott nor Dexcom have disclosed pricing for the upcoming products. In April 2024, Dexcom’s outgoing CEO Kevin Sayer said Stelo “pricing is going to be competitive” with other cash-pay products.
Around that time, William Blair analysts said Abbott’s cash-pay price for its Freestyle Libre CGMs was about $80 per month.
In the U.K., where Abbott first launched its Lingo device, the company charges about 120 pounds per month (roughly $152). “While some pricing data is available in that market, management suggested it may not be reflective of domestic pricing,” Kaczor Andrew wrote in a Monday research note.
Abbott’s Lingo CGM is not intended for people with diabetes. For wellness purposes, such a device can still be useful if it helps people see how their blood sugar reacts to food and activity, Stanford Medicine endocrinologist Marilyn Tan said.
Courtesy of Abbott
Why might people who don’t take insulin use a CGM?
Marilyn Tan, an endocrinologist with Stanford Medicine, said that while early CGMs were intended for patients on insulin, “increasingly, patients not on insulin are using CGMs.”
While hemoglobin A1c levels are a standard measurement of glycemic control, tests only provide an average over three months, Tan wrote in an email. She added that CGMs can provide minute-to-minute data and details on how that average was achieved.
“Particularly for diet-controlled patients and patients not on insulin, having a CGM can give important feedback about which foods raise their [glucose] and which do not, and each person reacts differently to different foods,” Tan said. “Therefore, this really allows for more individualized diet recommendations.”
For people with prediabetes, seeing this data can also be helpful and be a good motivator to make lifestyle changes. “As for ‘wellness,’ if someone does not have diabetes or prediabetes, it may be interesting to see glycemic excursions related to food and activity, and if it motivates them to improve their health, then it [can] be a useful tool,” she said.
William Blair’s Kaczor Andrew estimated that 700,000 to 800,000 people in the U.S. who don’t take insulin already use CGMs.
What software features set these apart from prescription devices?
Dexcom’s Leach said Stelo will include “quite a few features in it that are brand new to CGM users.” The app is designed to onboard people who have never used a CGM, as well as to educate them about what blood glucose means and how changes throughout the day are normal. The product’s main purpose is to help people manage their diet and activities to lower their average glucose, Leach said.
“We do expect that a large number of people are going to try [Stelo] that don't have diabetes."
Jake Leach
COO of Dexcom
Abbott’s Lingo “tracks glucose and provides personalized insights and customized coaching to help people create healthy habits, retrain their metabolism and improve their overall well-being,” a company spokesperson wrote in an email.
Lingo will provide minute-by-minute glucose data, specifically focusing on patterns after food intake and exercise, J.P. Morgan analyst Robbie Marcus wrote in a research note.
Abbott shared less detail about its upcoming Rio device. Marcus expects it will have a more targeted software interface than the Libre 3, and will not have the alarms or notifications needed by people who take intensive insulin.
“This is also one of the most annoying features for patients, so it’s great to remove them for a patient group that doesn’t really need them,” he wrote.
BTIG analyst Marie Thibault expects the device won’t include an alarm system and will have more of a consumer angle. She also said Rio can measure a wider blood glucose range of up to 400 mg/dL, compared to Lingo, which caps at 200 mg/dL.
Over-the-counter CGMs, such as Dexcom’s Stelo, use similar hardware to their prescription counterparts. The main difference is in software features, such as more education around time in range and a lack of alarms.
Courtesy of Dexcom
Why did Abbott and Dexcom take different approaches?
Abbott will offer two different over-the-counter CGMs because “there’s no one size fits all approach to managing care,” a company spokesperson wrote. For example, people living with diabetes might want features for insulin management, medication tracking and sharing data with a provider or caregiver, while people looking to better their overall health and wellness might need different features, the spokesperson wrote.
Dexcom is currently just offering one over-the-counter CGM. While Stelo is intended for people with Type 2 diabetes, “we do expect that a large number of people are going to try it that don't have diabetes,” Leach said.
After launching Stelo, Dexcom plans to iterate on its learnings to meet the needs of a broader group of users. Whether that means launching a separate device, like Abbott, is yet to be determined.
“We haven't quite decided exactly how that's going to go,” Leach said. “It really depends on how different the users’ needs are.”
Dexcom has estimated it will see $40 million in sales this year from Stelo. Abbott declined to share sales projections, Marcus wrote. He added that Abbott expects its diabetes business to grow to $10 billion in sales by 2028, which includes sales from Libre Rio but does not factor in Lingo.
Abbott CEO Robert Ford first announced the Lingo line of products at CES in 2022. The company hopes to make $10 billion in sales from its Libre line of CGMs by 2028, not including Lingo.
Ethan Miller via Getty Images
Will OTC devices make CGMs more accessible?
Stanford’s Tan said over-the-counter products may not necessarily lower the cost of CGMs because insurance should cover the devices for patients taking insulin.
“Without insurance, CGMs can be quite expensive even with patient assistance programs and coupons,” Tan wrote in an email. “I don't yet know how expensive the OTC CGMs will be, but they may not actually be cheaper than obtaining it through a prescription.”
On the other hand, insurance often doesn't cover CGMs for people with Type 2 diabetes who don’t take insulin, Joshua Neumiller, president-elect for healthcare and education at the American Diabetes Association, wrote in an email. “OTC CGM availability will help address access barriers for these individuals,” he added.
“I don't yet know how expensive the OTC CGMs will be, but they may not actually be cheaper than obtaining it through a prescription.”
Marilyn Tan
Endocrinologist at Stanford Medicine
Since the devices are FDA-cleared, people can use their health savings and flexible savings accounts to purchase them, the Abbott spokesperson wrote.
“Many people with diabetes already have coverage for our FreeStyle Libre system, and we’re continually looking to expand this coverage to help more people with diabetes get access to the technology,” the spokesperson added.
Is there a concern that people will use an OTC CGM when they need a prescription CGM?
BTIG’s Thibault said there’s some risk, but since prescription CGMs are well-covered by insurance, people would probably pay more to get them over the counter.
“The label is saying you aren't going to be dosing insulin off of this,” she said. “There's a little bit of risk that someone would use it in that way, but it's certainly off-label use and the market structure today disincentivizes those insulin users because they could get coverage another way.”
ADA’s Neumiller said a prescription CGM would be more appropriate for people taking insulin, who have a history of problematic glycemia or who could benefit from integrating their CGM with insulin pumps or other devices.
“It will be important to educate people with diabetes about the key functional differences between over-the-counter CGM and prescription CGM products,” Neumiller added.
Are other CGM-makers, such as Medtronic, likely to sell an OTC device?
Other companies might eventually pursue over-the-counter CGMs, but Thibault doesn't expect to see new entrants in the next 12 to 18 months.
“I don't see many companies that have the footprint today in CGM and the investment dollars to make that work,” she said, adding that Abbott and Dexcom currently dominate the market for disposable CGMs.
Article top image credit: Courtesy of Dexcom
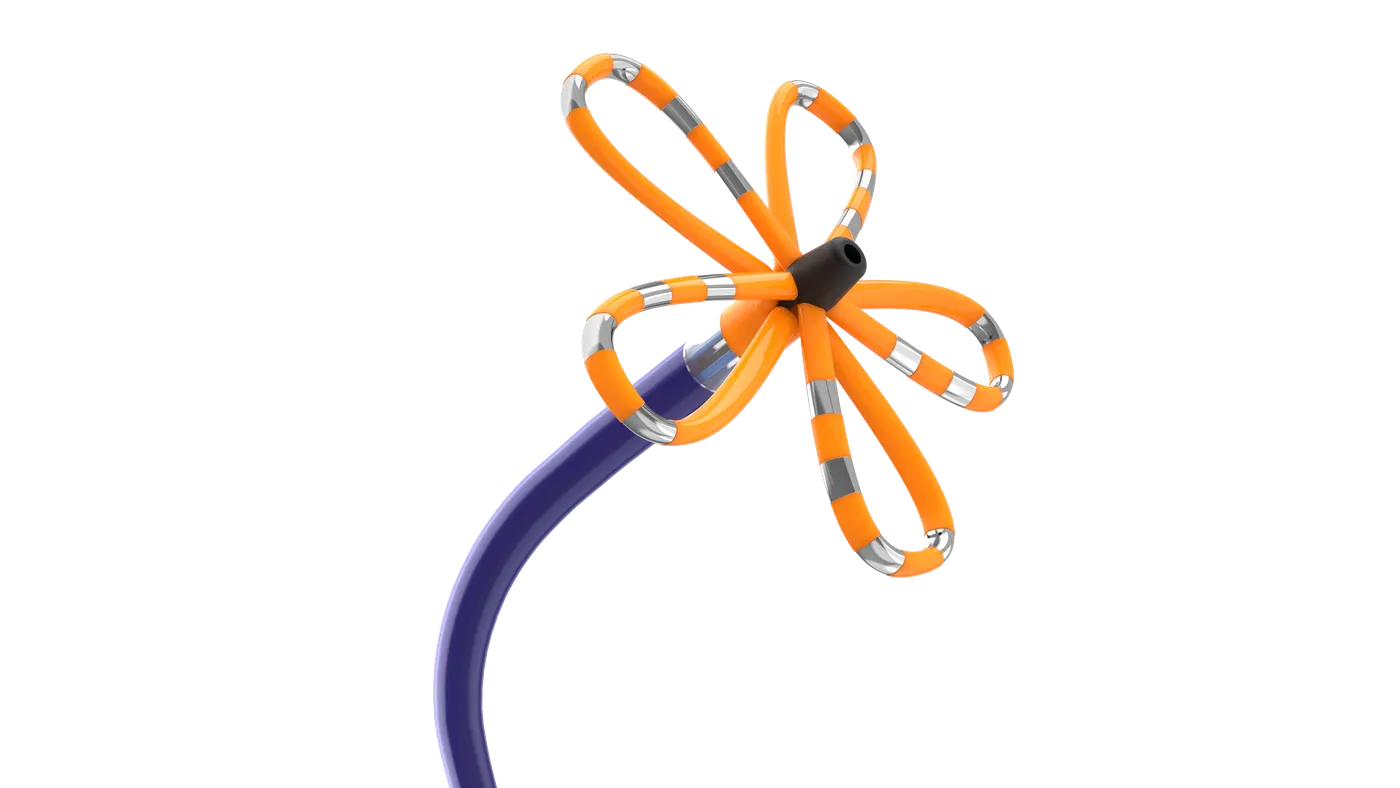
PFA devices are changing AFib treatment. The next wave could grow the market further.
New pulsed field ablation systems from Boston Scientific and Medtronic are already reshaping the cardiac ablation market, but upcoming devices could spur even greater adoption.
By: Susan Kelly• Published June 17, 2024
A new technique for treating patients with a common heart arrhythmia is rapidly replacing traditional methods in one of medtech’s biggest new developments.
Atrial fibrillation, the heart rhythm disorder, affects 50 million people worldwide, yet less than 5% of those who could benefit from a cardiac ablation procedure to address itnow get treated, according to Jasmina Brooks, president of Johnson & Johnson’s Biosense Webster subsidiary.
Heart device makers including J&J believe they have a solution to narrow that gap, a procedure called pulsed field ablation. The technology has sparked tremendous buzz among heart specialists and Wall Street analysts, who predict speedy adoption of the new technique.
“We believe that PFA will expand that market and hopefully help us improve that less than 5% number and improve the access for people who are impacted by AFib. That's probably the biggest benefit that we expect from PFA,” Brooks said in an interview.
AFib causes the heart to beat inefficiently, increasing the risk of stroke or heart failure, and its prevalence is growing as the population ages. Drugs don’t always work to restore normal heart rhythm in AFib patients. PFA promises faster procedure times than traditional ablation methods and may be safer for patients.
PFA applies nonthermal energy to correct faulty electrical signals in the heart. A catheter targets specific heart cells with high-voltage electrical pulses, reducing the risk of injury to surrounding tissue.
The technology differs from older techniques like radiofrequency ablation, which uses heat to scar heart tissue and block abnormal signals that cause AFib, and cryoablation, which uses extreme cold to target tissue.
“Physicians both in the U.S. and [outside the] U.S. are excited to try the innovation,” Brooks said. “They're excited about the promise of safety, efficiency, workflow efficiencies as well. Those continue to be really key considerations to adopting the new technology.”
The first PFA systems to hit the U.S. market — Boston Scientific’s Farapulse and Medtronic’s Pulseselect —started rolling out in 2024. Boston Scientific’s Advent pivotal trial was a tipping point for the industry, according to analysts, when the results last fall showed PFA to be as effective as RFA and cryoablation, and potentially safer.
“There is the belief that it's safer and that was supported by the Boston trial, which was a head-to-head trial with RF ablation, and then there was a secondary safety endpoint where it showed it was superior,” said Needham analyst Mike Matson.
Shorter procedure times are a big part of the technique’s appeal, allowing doctors to increase their case volumes. “That throughput matters a lot to hospitals,” said BTIG analyst Marie Thibault.
‘Very rapid’ uptake
Boston Scientific CEO Mike Mahoney touted Farapulse as a “transformational” product for the company in a 2024 earnings update. The CEO pointed to a “very rapid” uptake from users of both RFA and cryoablation.
Mahoney declined to disclose initial sales figures for Farapulse, which was launched midway through the first quarter of 2024. However, BTIG’s Thibault thinks revenue from the device could have reached $40 million to $50 million in that short time.
“It is a very high number, certainly the most successful medical device launch that we can think of,” Thibault told MedTech Dive.
Before PFA, radiofrequency energy was the preferred approach in roughly 85% of AFib ablation procedures, said Thibault. Meanwhile, cryoablation comprised about 15% of cases.
After Boston Scientific’s Advent data were released, BTIG surveyed 25 heart doctors who on average expected to shift half of their AFib procedures to PFA in three years. Thibault predicted that number could be closer to 60% because the technology now appears headed for even faster adoption.
Like Boston Scientific, Medtronic has reported high interest in its PFA technology, with cardiovascular group President Sean Salmon citing “astonishingly great” demand on the company’s earnings call in May 2024. Medtronic was first out of the gate in the U.S. with a December 2023 approval for Pulseselect.
Medtronic executives also were mum on PFA sales, but CEO Geoff Martha said the products drove 21% sequential growth in the company’s cardiac ablation business in its fiscal fourth quarter, as the technology more than offset declines in its cryoablation line.
Mapping the procedure
J&J, which filed an FDA submission in March 2024 for its Varipulse platform, is on track to become third to the U.S. market with a PFA system that will likely launch later in 2024, said RBC Capital Markets analyst Shagun Singh. J&J expects the integration of Varipulse with its Carto heart mapping system to distinguish its PFA offering from the competition.
Mapping helps physicians determine where to ablate before the procedure and confirm the results afterward. J&J has a huge installed base of mapping systems, said Singh.
Boston Scientific is looking to integrate mapping with PFA in 2024, and Medtronic recently filed for U.S. approval of its Affera mapping and ablation system.
Abbott also has a mapping system on the market but is lagging in the PFA race. The company announced in January 2024 that it completed the first procedures in a study of its Volt PFA device and expected to receive approval to start a U.S. clinical trial, leading analysts to predict the system could be introduced in the U.S. in 2026. It began enrolling patients in the U.S. study in April 2024.
With PFA rollouts and more expected approvals shaking up the competitive landscape in AFib treatment, the electrophysiology market “is going to be very dynamic for the next two to three years,” said Singh.
Device makers overall have continued to post strong revenues from radiofrequency procedures, said BTIG’s Thibault, noting the enthusiasm around PFA is “lifting all boats for ablation in general.”
Article top image credit: Permission granted by Boston Scientific
More than 1,100 devices have received the FDA’s breakthrough designation
The FDA updated its list of breakthrough devices as medtech groups lobby for faster Medicare coverage of products with the designation.
By: Elise Reuter• Published Aug. 21, 2025
A total of 1,176 products have received the Food and Drug Administration’s breakthrough device designation since 2015, according to the agency’s latest update in August 2025.
The FDA gives the designation to devices that may provide more effective treatment or diagnosis of life-threatening or debilitating conditions. In its 2025 fiscal year, which began in October 2024, the agency had granted 136 breakthrough designations as of June 30, 2025.
During the first Trump administration, the Centers for Medicare and Medicaid Services finalized a rule that would prove near-automatic Medicare coverage for four years for FDA-authorized breakthrough devices. Under the Biden administration, CMS quickly scrapped the rule over concerns about the lack of clinical evidence, saying it would result in “premature coverage of unproven devices” for seniors.
In the FDA’s 2024 fiscal year, the agency granted breakthrough status to 165 devices, according to the latest data. Although breakthrough devices cross all specialties, the majority were in cardiovascular, neurology and orthopedics.
Some of the latest breakthrough devices authorized by the FDA include a bone graft for lumbar fusion procedures. The product, called PearlMatrix, was approved by the FDA in June 2025 following a 293-person randomized controlled trial.
Another recent example is Intuitive Surgical’s X and Xi robots. Intuitive received 510(k) clearance in June 2025 for an expanded indication for tracheobronchoplasty, a procedure for people whose trachea is soft and can collapse. Intuitive presented real-world evidence from a database as part of its application to the FDA.
Article top image credit: Sarah Silbiger via Getty Images
How CMR Surgical is taking on robotics’ ‘800-pound gorilla’
“I don’t think a monopoly market is healthy,” said CMR co-founder Mark Slack, discussing robotic surgery pioneer Intuitive Surgical’s continuing dominance in the market.
By: Susan Kelly• Published Dec. 3, 2024
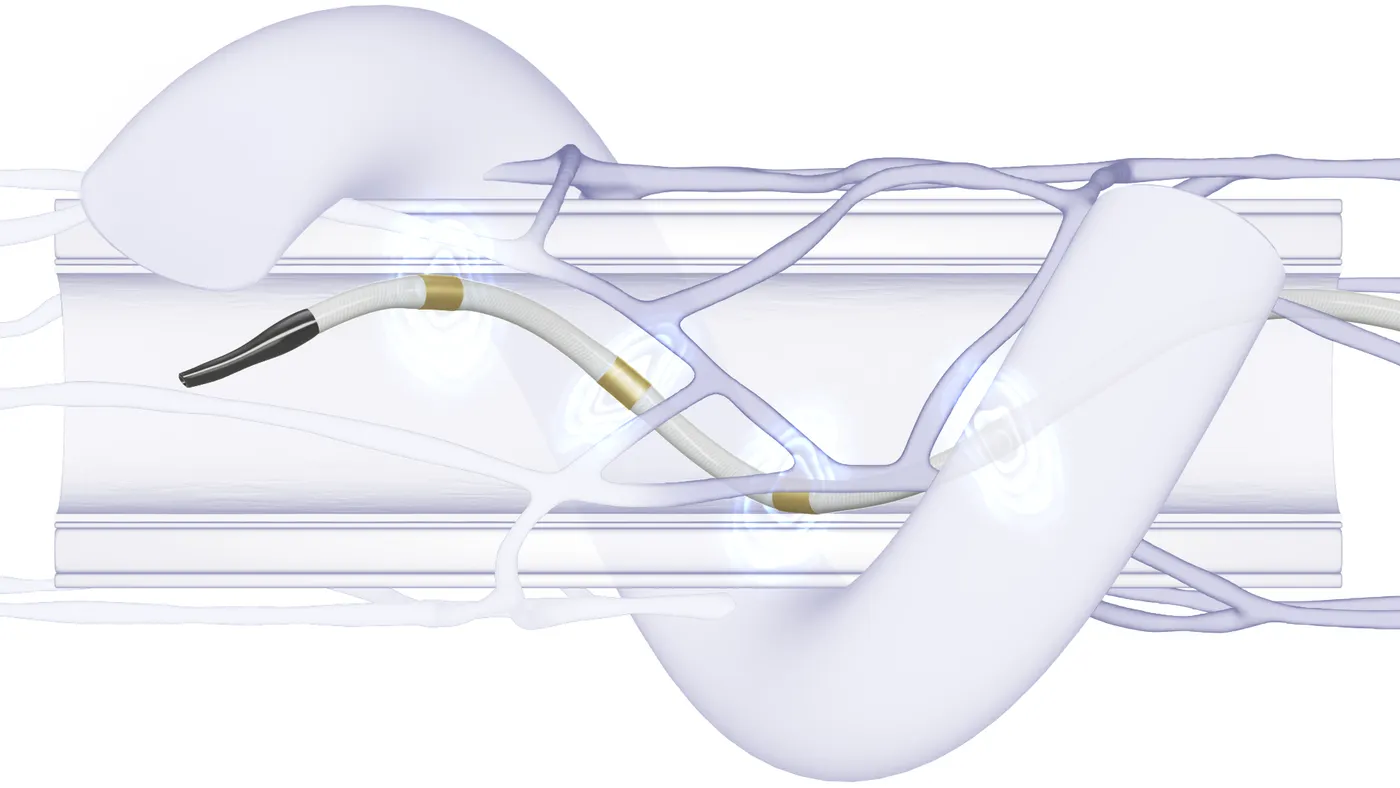
CMR Surgical is taking on Intuitive Surgical in the U.S. after gaining a de novo authorization in October 2024 for its Versius robot, challenging the market leader’s 20-year dominance in soft tissue robotic surgery.
In competing with Intuitive on its home turf, UK-based CMR has pulled ahead of Medtronic and Johnson & Johnson, whose soft tissue surgical robots are not U.S.-approved. Versius’ first indication is in gallbladder removal surgery, with more procedures expected to follow.
“This competition, it’s good for health. I don’t think a monopoly market is healthy,” said Mark Slack, CMR co-founder and chief medical officer. “There will be 3-4-5-6-7 providers in due course.”
Slack said users are attracted to the Versius robot’s flexible design and smaller-sized instruments. He is not fully sold on force feedback sensing as a robot advantage and would like to see more data in general on how well surgical robots are performing. CMR’s robot will also compete on price, Slack said.
Slack discussed the Versius system’s attributes and the advantages and challenges of robotic-assisted surgery in a conversation with MedTech Dive.
This interview has been edited for length and clarity.
MEDTECH DIVE: Why did you choose to introduce Versius in multiple global markets before focusing on the U.S.?
MARK SLACK: Largely picking a fight we could win. There's an 800-pound gorilla in the room called Intuitive. It is uniquely successful. Not ever in medtech has there been a single company that’s had such a monopoly on any subject.
They brought the robot out in [2000], and the first robot to compete with them, the first competitor, was us in 2019. So they're 20 years just running. To go head-to-head with them in their own backyard is pretty damn dangerous. And so, we wanted to get established. We wanted to do more clinical development.
I also have a great belief that if you are going to be successful with medical technology, it's got to be not just for the high-income countries. If we’re saying that's the best standard of care, then that should be hopefully translated to all other communities around the world. That's where I started. But you can't stay out of America with health. So yeah, time to join in.
I don't think Intuitive will be particularly delighted with us coming.
How will Versius compete against Intuitive’s da Vinci?
It's a smaller robot, it's modular, it's more transportable. It can be packed out of the way when not using it. The modularity and affordability are really important.
When you have six, seven or eight robots in a hospital, which is the way it's going, where do you put them, if they're very big, when you're not using them? You actually close theirs down when you're not using them, whereas ours can be put against the wall, in a cupboard, etc. It's easier to store and therefore doesn't occupy large amounts of space in a hospital or shut down your theaters.
From the point of view of staff being open, being able to talk and communicate, the modularity is hugely important. The nurses 100% want to be in interaction with the surgeon, and the anesthetists want their open console.
And then finally, we have smaller instruments than the other robots, and that means that we perform pretty well in small spaces.
Ultimately, we will compete in all operations, but there will be areas where we really do shine, like the chest, or in children, where the anatomical spaces are smaller, which actually favors the smaller robot.
Do you expect some hospitals to add a Versius robot while also continuing to use da Vinci?
We see it already. We have a number of hospitals in the UK that have both, and some surgeons like the one and others like the other one. That still is a war that needs to be played out.
It's unlikely that you'll ever get an instrument that everybody thinks is the best, and there will be strengths and weaknesses. Over time, as we play it out, and as we do more research and we get the data, we'll see where we absolutely shine, and we'll see areas where we are equivalent, and then possibly areas where it might be superior.
You notice I said might.
We have some centers where people have done 1,500-2,000 cases on our robot and really gained extensive experience. We have some users in the U.S. who are genuinely waiting for us because they feel we are the right size. They are very keen that that might be a better way of doing robotic surgery.
We've got to be sure of what's real in terms of advantages and what's not. We actually have force feedback on our robot, and we choose not to activate it at the moment. I'm partly the reason for that. I'm not 100% convinced that it does improve things.
I think force feedback has a way to go to be really useful. And you know how many hundreds of thousands of cases have been done robotically with outcomes better than laparoscopic surgery with no force feedback, and that's the da Vinci figures.
And then all the other features, it's how much of it is marketing and how much is real? And that's what I would like to see more in robotics: less hype and more fact. What is the satisfaction rate? What is the success rate? What are the false negatives and the false positives and so on. Those are all really, really important things that we need to be a little bit more medical about as we go forward. Otherwise, the whole health system just becomes more and more expensive and not necessarily better.
Is robotic-assisted surgery better than laparoscopy?
That's a very important point to decide. If you asked me, at the moment, to debate that robotics is better than laparoscopy, I would be pretty cautious. If you take a really skilled laparoscopic surgeon, the chance that the robot will necessarily do it better than them is quite slight, because they are fast, they are able, and they are very good at it.
However, we are now starting to see data from areas where the robots are performing better than laparoscopic [surgery]. Watch the space. I think you may well find superiority in robotics over laparoscopy.
I believe I can train a person on robotic surgery far quicker than I can train a person for laparoscopy, and better. We’ve got data to support that. If I was going to teach you — you may be a very skilled laparoscopic surgeon — to tie a knot laparoscopically, that's about 50 or 60 hours worth of training. I reckon on a robot I could teach you in about an hour.
If I had a crystal ball, in 10 years time, I think we will be showing the advantages of robotics over laparoscopy.
What other indications are you pursuing, and how is that process going?
We chose to go in the most efficient route possible, both financially and time-wise, which is to do a de novo and therefore only chose limited clinical indications. The idea being, once we get that, we'll then [submit 510(k) applications] on multiple other clinical scenarios. We'll start by upgrading the system, and then we'll do colorectal, thoracic and all the other specialties, one after the other.
The real achievement was getting the system past a full FDA approval for the system and for all our instruments, because then doing the 510(k) is altogether much easier. So we do small, limited clinical trials and expand it across to the other specialties here.
Article top image credit: Permission granted by CMR Surgical
Why HCA is ‘all in’ on surgical robotics
Thomas Payne, HCA Healthcare’s national medical director of robotics, explains how the largest U.S. health system is vetting a new crop of market entrants.
By: Susan Kelly• Published March 24, 2025
As the national medical director of robotics for HCA Healthcare, Thomas Payne is on the front lines of the revolution in robotically assisted surgery.
Payne works with HCA’s surgeons to choose which robots will be used in the health system’s facilities, determining the best technologies to acquire from a rapidly expanding field of candidates.
The country’s largest for-profit hospital operator now employs about 20 different robotic platforms across its centers, or a total of 933 robots as of February 2025. The robots have helped perform more than 1 million surgical procedures at HCA facilities, a milestone reached in 2024, according to Payne.
The surgeon executive spoke to MedTech Dive about the reasons for the increasing use of robots in surgery, why HCA has fully embraced the robot-assisted approach, and how the healthcare provider evaluates new entrants to a market long dominated by Intuitive Surgical.
This interview has been edited for length and clarity.
MEDTECH DIVE: How does HCA think about its investment in robotics?
THOMAS PAYNE: We’re all in. The patient is our mission. The partners are the surgeons. We like to say we don't just buy robots, but we build robotic programs.
When new robotic platforms come out, we'll have a board of physicians or surgeons or experts in that facility give us feedback and say, “Hey, that's a valuable piece of technology. We think that will help us take better care of our patients.” Or, “It's not ready for prime time.”
How do you decide which robots to buy?
Our surgeons pick the winners. There's not an administrator picking the winners or board picking the winners. It's our surgeons that give us feedback.
We do more robotic surgery than anybody in the world. Because the volume is so high, we built our robotic program very methodically. Getting into robotic surgery is expensive, so you have to run a program efficiently to take the best care of your surgeons and your patients and not be too expensive.
We're convinced that the total cost of healthcare comes down with robotic-assisted surgery.
Is robotically assisted surgery better for patients?
All the bad things that you don't want to happen in surgery happen more often with open surgery. Clinically, in some cases, you have to do open surgery. You just have to. There's no choice. But in general, probably 95% of all surgeries out there can be done minimally invasive, if you have the right skill set, the right robot and the right program.
Our goal is to perform almost all minimally invasive surgery. Our surgeons want it because they know it's better for their patients. Things like complications, blood loss, transfusions, readmissions, long lengths of stay in the hospital, infections — all those things are much higher with open surgery than they are with minimally invasive surgery. And robotic-assisted surgery is the most reproducible way to do minimally invasive surgery.
Almost all of our facilities are at somewhere less than 10% open surgery. That's a paradigm shift. As a surgeon or physician, you want to be alive in your career when something exciting happens, like antibiotics, or radiation, or chemotherapy, or something that really is a game changer. In the surgical space, robotic-assisted surgery is that paradigm shift.
And with the new computational powers that are coming into the new systems, now you're talking about cycles of improvement with AI and all the different things that are going to be put on top of that, to keep surgeons optimized in their skill sets. You're going to see more of that come in, and it's just going to speed up and get even more dramatic over the next five to 10 years.
How is the field of surgical robotics evolving?
HCA is in the graduate medical education space as well. We are the biggest trainer of residents in the world. All the surgical residents in HCA hospitals go through advanced robotic courses in their junior year. They get robotic-certified, so when they graduate, they're ready to go.
The change I've had the privilege of seeing in my career, which was taking arrows in the back in the early days when doing robotic surgery was very controversial – now, when I ask those residents for a show of hands: “How many of you are looking for jobs after you graduate in hospitals that don't have robotics?” Crickets. It's almost like they have to have robotic-assisted surgery, or they don't want to go to that hospital. That is their preferred way of operating now.
That's very, very different than when I trained in the 1990s, or very different than even 10 years ago.
There’s a lot of competition coming in surgical robots. How do you assess them all?
I have a PowerPoint slide that has all the company names of all the robots that are either FDA-approved or soon-to-be, and it's literally 100. It's coming so fast and so quick. Not all of them are going to be successful soon. In fact, the majority are not going to be successful. They'll probably never get out and gain traction.
As this country's largest healthcare company, they all want to get in front of us, to show us what they have. When they get a handful of surgeons interested in their product, then we'll start listening.
We get six or 10 experts in robotics to go and look at that new product. If we have surgeons that are interested, we're willing to purchase or place those robots in our hospitals, but then they better be successful, and they better be used, because we're not going to go down the road with the technology that doesn't compete at a high level with what's already established.
We talked to J&J, we talked to Medtronic, we talked to Virtual Incision’s Mira, we talked to Endoquest. We talked to all the different types of robotic platforms — orthopedic, pulmonary, spine, neuro – all those companies we spent a lot of time talking with.
If we have enough surgeons that are interested in that technology, we go kick the tires, so to speak. Then if we get to the next level where surgeons come back super excited, like this is amazing, we really need to have this, then we'll go with that. And then we'll check again right after we buy two or three or four or five. Then we're going to check again and make sure that is consistent.
We're just trying to be good stewards of our resources, because if we waste resources over here, that's just money that we can't use to take care of patients over here. So we're pretty good stewards and pretty frugal, I would say. There's a plan on robotic purchases, and we follow those business plans pretty religiously. And so far, it's been really successful for us.
Article top image credit: Permission granted by HCA Healthcare